Blog
Why Bridge is a charting stickler
Most virtual care companies treat charting as a checkbox. Bridge treats it as the foundation of trust. Rigorous audits turn documentation into proof of quality, improving care, earning payer confidence, and unlocking coverage at scale.

.png)
Executive summary
- Bridge's chart auditing program starts with one priority: exceptionally high quality patient care. When you get that right, health plan trust follows almost immediately and state regulations are more than satisfied along the way.
- Virtual care's ability to reach underserved patients and earn health plan coverage depends on a demonstrated, documented quality standard. Chart auditing is how that standard gets built.
- Bridge reviews 5% of all partner charts monthly using licensed, specialty-credentialed auditors across both chart completeness and clinical decision-making.
- The result is a consistent quality bar that holds across all 50 states, improves measurably over time, and gives health plans the evidence they need to cover virtual care with confidence.
Bridge has developed a reputation among our partner clinics for being demanding about documentation. During onboarding, we share note templates and review provider notes once the integration is complete. Most clinics come in with a minimal audit program, or none at all. We expect that. It's part of why Bridge's audit infrastructure exists: so that the clinical quality work doesn't depend on what a partner has already built, because in most cases, they haven't had the time or resources to build much. For a virtual care company focused on growth, standing up a rigorous chart audit program is rarely the first priority. Bridge builds that infrastructure so our partners don't have to.
The reason we operate this way is worth explaining, because it goes well beyond compliance. State regulations are the floor, and Bridge meets them, but only 12 states require nurse practitioner chart audits, and most of those laws are written loosely enough that a virtual care company can technically comply while running a program that catches almost nothing. That's not what we're after.
What we're after is trustworthy virtual care. Virtual care has enormous potential: to reach patients in underserved geographies, to provide more flexible access to specialists, to deliver care at a cost and convenience that in-person settings can't match. But potential and realized value are different things. One element necessary to realizing that goal is that health plans trust the care enough to cover it on the same terms as the in-person care they've spent decades evaluating. Chart auditing is a significant part of how that trust gets built.
Why we do this in the first place
Bridge's mission is to expand trustworthy virtual care across the country. The word "trustworthy" points in two directions at once: toward health plans, who need to trust the care enough to cover it, and toward patients, who need to trust that the care they're receiving is actually good. Chart auditing serves both, but providing quality care for patients is our primary driver.
A thorough chart is a communication tool as much as a compliance document. When a provider documents the reasoning behind a prescription, the clinical judgment applied to what a patient reported, the chart becomes something the entire care team can use. A colleague picking up the same patient six months later has context. A specialist consulted on a complex case isn't working blind. Documentation makes continuity of care possible, and continuity of care makes better health outcomes possible.
No patient has ever sat in a virtual visit thinking about whether their provider is documenting their diagnosis with appropriate specificity. But better charting produces better care, and better care produces healthier patients. The audit program operates invisibly to patients. Its effects don't.
When patients receive high quality care consistently, health plans notice. A virtual care partner with clean charts, strong audit scores, and a track record of clinical rigor is a partner health plans can send their members to with confidence. Quality, in that sense, is what makes the partnership work.
The challenge health plans are navigating
Health plans know in-person care deeply. They've spent decades building frameworks to evaluate it, contract around it, and measure its quality. They know what good documentation looks like, what appropriate utilization patterns look like, what a well-run primary care practice looks like when they audit it. Virtual care is newer territory. The care model works differently, the documentation looks different, and the benchmarks health plans use to assess quality in a traditional clinic don't always map cleanly onto a virtual visit.
When a health plan agrees to cover virtual care for its members, it's making a meaningful bet: that those members will receive care that meets the same standard of quality they'd receive in person. A health plan's job is to make responsible, evidence-based coverage decisions, and they're right to ask hard questions before making them. What chart auditing provides is the answer to those questions, grounded in actual documentation that holds up to professional review rather than marketing materials or founder testimonials. When the chart is clean, with the diagnosis documented with appropriate specificity, the clinical rationale made explicit, and the right flags raised, that's evidence a health plan can evaluate on its own terms, visit by visit, until the track record speaks for itself.
Three types of audits, three different jobs
There are three distinct types of audits that matter in virtual care: chart audits, clinical audits, and billing audits. Bridge's clinical quality program is built around the first two. Billing and coding accuracy is handled separately by Bridge's in-house billing team, which runs its own audit processes with its own rigor. The distinction between chart and clinical audits is where most virtual care companies have the biggest blind spots.
A chart audit is about documentation completeness. Did the provider capture what happened in a way that's legible, thorough, and defensible? Is the diagnosis recorded with appropriate specificity? Is there a documented plan? Could another provider read this chart and understand exactly what happened without calling anyone? The question concerns the record, not the quality of the care: does the documentation reflect what was done?
A clinical audit is a different job. The question is whether the clinical decisions met the standard of care, defined as what the medical community would recognize as appropriate for this patient, at this point in their care. A menopause patient is prescribed estradiol without progesterone. If that patient has a uterus, unopposed estrogen raises endometrial cancer risk; standard of care requires progesterone alongside it. The chart doesn't document uterine status. The auditor can't confirm whether the prescription was appropriate or whether a critical piece of patient history was missed entirely. That kind of review demands genuine clinical breadth. Bridge's auditors move across specialties within a single afternoon's work.
The two catch different things, but a chart that fails a documentation audit usually has a clinical gap somewhere, and vice versa. Bridge treats both as equally important, and our program is built to handle both within the same review.
What chart auditing actually does for care quality
Bridge reviews 5% of all charts manually each month, using licensed and board-certified reviewers with specialty-relevant expertise. That 5% follows an algorithm rather than random selection: every provider receives a review each month, with charts sampled proportionate to volume, so more active providers receive more scrutiny.
The sampling methodology is the mechanism. The relationship between auditor and provider is what makes it work. Bridge's approach to chart auditing borrows from the same Just Culture framework the aviation industry adopted decades ago: the goal is to catch where the process broke down, understand why, and fix it before it happens again, rather than to assign blame to individuals. Erin Flynn, Bridge's VP of Clinical Quality, is a clinician herself, and she's deliberate about how her team positions the audit relationship. Nobody improves when they feel surveilled. Providers who feel like internal affairs is watching them get defensive; they don't get better. The audit has to land as a fellow clinician helping them do excellent work, and Flynn runs her program accordingly.
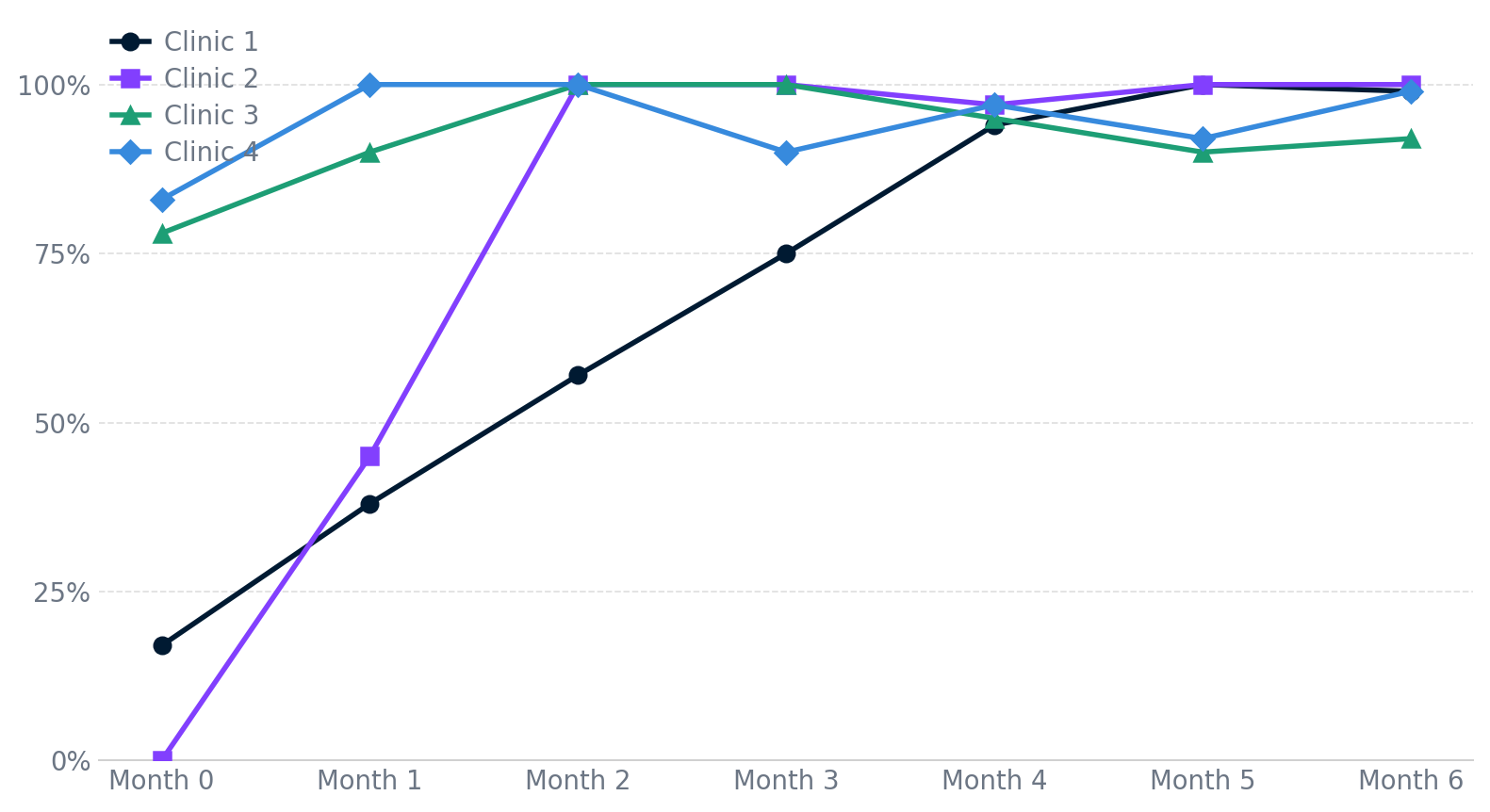
Clinics that come into Bridge's program with low chart audit scores don't stay there. The chart below shows audit pass rates for four clinics over their first six months in Bridge's program, each starting from a different baseline, all converging toward the same standard.
The program works because the feedback is real, the reviewers are credentialed, the posture is collaborative, and the bar is the same for every provider in every state.
Trustworthy care is how virtual care scales
Bridge's audit program comes built into every partner relationship, designed to a consistent standard across all 50 states. For health plans, that means the virtual care partners in Bridge's network are actively monitored, findings are acted on, and the quality bar holds whether a member is in Indiana or Oregon, whether the provider joined the network last month or six years ago.
That consistency matters more than it might first appear. Demonstrating quality is the harder problem in virtual care, and demonstrating it at scale, in a form that health plans can evaluate with confidence, is harder still. A rigorous audit program run uniformly across every partner relationship is how that proof gets built, and how a virtual care company moves from being an unknown quantity to a verifiable partner. A verifiable partner is one health plans can confidently send their members to, and one positioned to grow.
The connection between quality and scale is direct. Virtual care has the potential to reach patients who can't easily access in-person care: rural communities, people with inflexible schedules, patients who've never had a nearby specialist available to them. That reach depends on coverage. Coverage depends on trust. And trust depends on the kind of demonstrated, documented, consistently reviewed quality that a serious chart audit program produces. What starts as documentation discipline ends, over time, as a larger network of people receiving care they wouldn't otherwise have access to.